La stimolazione magnetica periferica ripetitiva (rPMS) è stata recentemente applicata con successo negli emicranici per alleviare i sintomi dell'emicrania. Il sollievo dai sintomi è stato ottenuto stimolando i punti trigger miofasciali (mTrPs) dei muscoli trapezi, che sono considerati parte del complesso trigemino-cervicale (TCC). Tuttavia, gli effetti sulla muscolatura non sono stati valutati in dettaglio e la specificità degli effetti sui muscoli considerati parte del TCC deve ancora essere chiarita. In questo contesto, questo studio presenta l'impostazione della rPMS nell'emicrania e valuta gli effetti sulla muscolatura scheletrica.
Materiali e metodi:Trentasette adulti (età media: 25,0 ± 4,1 anni, 36 femmine) affetti da emicrania e che presentavano mTrP all'esame obiettivo sono stati sottoposti a rPMS o a mTrP nel muscolo trapezio (considerato parte del TCC;
n = 19) o nei muscoli deltoidi ( considerato non parte del TCC;
n = 18) durante sei sessioni nel corso di 2 settimane. Sono stati compilati questionari standardizzati per valutare eventuali eventi avversi e l'esperienza con rPMS, nonché la soddisfazione e i benefici della stimolazione. L'algometria è stata eseguita per valutare i cambiamenti nelle soglie del dolore da pressione (PPT).
Risultati:Tutte le sessioni di stimolazione sono state eseguite con successo senza eventi avversi, con l'84,2% dei soggetti del gruppo trapezio e il 94,4% dei soggetti del gruppo deltoide che descrivevano la rPMS come confortevole (
p = 0,736). Il dolore o la tensione muscolare sono migliorati nel 73,7% dei soggetti del gruppo trapezio e nel 61,1% dei soggetti del gruppo deltoide (
p = 0,077). I PPT dei muscoli del trapezio sono chiaramente aumentati dalla prima all'ultima sessione di stimolazione, indipendentemente dal muscolo stimolato (rPMS al trapezio o ai muscoli deltoidi). Tuttavia, a seconda dei muscoli esaminati, l'aumento dei PPT differiva significativamente (soggetti con stimolazione del muscolo trapezio:
p = 0,021; soggetti con stimolazione del muscolo deltoide:
p = 0,080).
Conclusione: rPMS è un metodo comodo negli emicranici che può migliorare il dolore o la tensione muscolare locale. Inoltre, è in grado di aumentare direttamente e indirettamente i PPT dei muscoli trapezi (considerati parte del TCC) quando applicato su mTrP, supportando il ruolo del TCC negli emicranici.
Tabe Renner 1,
Nico Sollmann 2 3,
Florian Trepte-Freisleder 1,
Lucia Albers 1,
Nina M Mathonia 1,
Michele V Bonfert 1,
Helene Konig 1,
Birgit Klose 1,
Sandro M. Krieg 4,
Florian Heinen 1,
Lucia Gerstl 1,
Mirjam N Landgraf 1 Affiliazioni
- 1Dipartimento di Neurologia Pediatrica e Medicina dello Sviluppo, Centro LMU per Bambini con Complessità Medica, Ospedale Pediatrico Dr. von Hauner, Ospedale Universitario LMU, Ludwig-Maximilians-Universität, Monaco di Baviera, Germania.
- 2Dipartimento di Neuroradiologia Diagnostica e Interventistica, Klinikum rechts der Isar, Technische Universität München, Monaco di Baviera, Germania.
- 3TUM-Neuroimaging Center, Klinikum rechts der Isar, Technische Universität München, Monaco, Germania.
- 4Dipartimento di Neurochirurgia, Klinikum rechts der Isar, Technische Universität München, Monaco di Baviera, Germania.
Figure 1 Setup of repetitive peripheral magnetic stimulation (rPMS). During algometry and rPMS, the subjects sat on a comfortable chair with armrests, headrest, and footplate in a relaxing position. Application of rPMS took place either to the myofascial trigger points (mTrPs) of the trapezius muscles (as shown in this case with the stimulation coil being placed on the left trapezius muscle with the help of a static coil holder) or to the mTrPs of the deltoid muscles depending on group assignment (trapezius group or deltoid group). The subjects were advised not to move during algometry or rPMS application and to rest in a relaxing position. Written informed consent was obtained from the subject of this figure to use this photo for publication.
Figure 2 Measurements of the pressure pain threshold (PPT) by algometry. Measurements of PPTs were performed with a handheld algometer, which was placed perpendicularly to the skin with increasing pressure until the subject indicated that the local PPT was reached. Algometry was carried out on all four myofascial trigger points (mTrPs) in each subject. Specifically, three consecutive PPT measurements were performed separately for the two mTrPs in the trapezius muscles and the two mTrPs of the deltoid muscles prior and subsequent to the stimulation of each session.
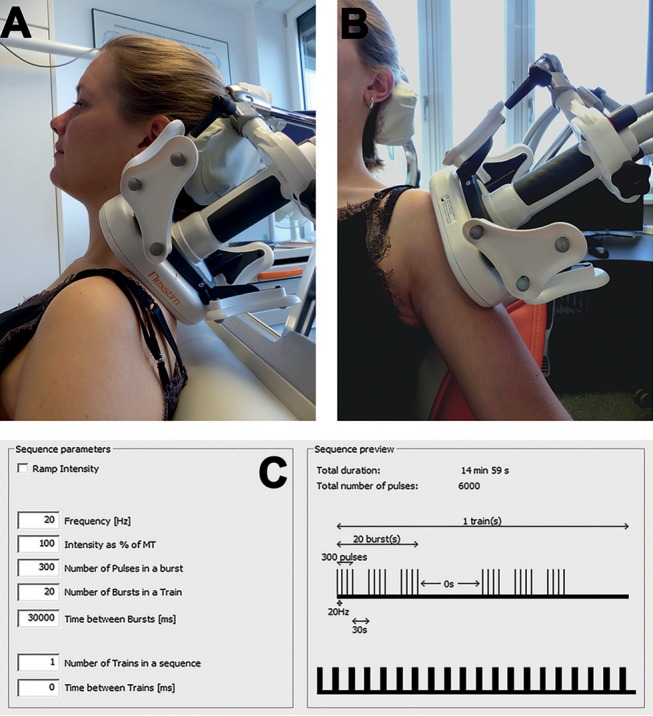
Figure 3 Stimulation by repetitive peripheral magnetic stimulation (rPMS). A figure-of-eight stimulation coil was used for rPMS, which was applied either to the mTrPs of the trapezius muscles (trapezius group) or to the mTrPs of the deltoid muscles (deltoid group) in the context of six stimulation sessions. Direct contact between the skin and the coil surface was ensured throughout, and the coil position was fixed by a static coil holder. In subjects of the trapezius group, the coil was centered and fixed above the previously identified mTrPs of the upper trapezius muscles perpendicularly to the anatomical course
(A). In subjects of the deltoid group, the coil was placed above the mTrPs of the deltoid muscles parallel to the anatomical course
(B). The stimulation protocol was the same in both groups (20 Hz) and took 15 min per side
(C). Written informed consent was obtained from the subject of this figure to use this photo for publication.